.
With the advance of vitreoretinal surgery, the above
physical signs are becoming more common in the clinical examination.
Always ask to examine the posterior segment for the
presence of previous retinal detachment, proliferative vitreoretinopathy
and advanced proliferative diabetic retinopathy.
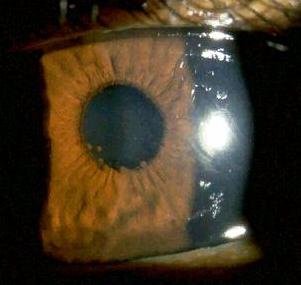
Silicone oil in the anterior chamber
The superior anterior chamber contains fine suspension
of silicone oil. The oil may appear milky owing to emulsification
(so-called inverted hypopyon).
Look for:
-
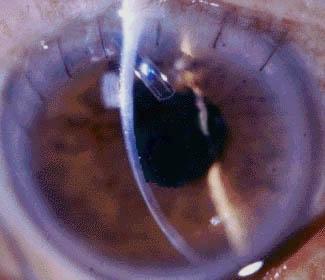
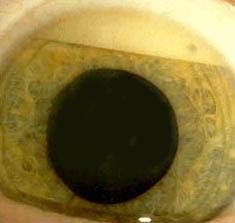
complications associated with the oil (ie. band keratopathy
and cataract)
-
presence of Anton's iridotomy (this is iridectomy performed
at 6 O'clock in aphakic patient to prevent
pupillary block)
-
previous retinal detachment
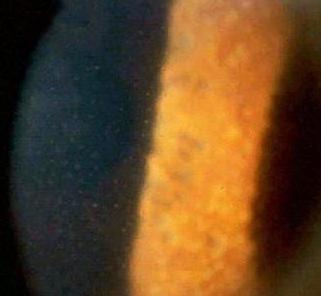
Heavy liquid in the anterior chamber
There are globules of liquid in the inferior part of the
anterior chamber.
Look for:
-
previous retinal detachment operation
. |