Like basal cell carcinoma, squamous cell carcinoma is associated
with sun damage and both conditions usually occur in the lower eyelids.
However, squamous cell carcinoma is far less common than basal cell carcinoma.
In the examination, you may be shown a clinical picture or slide of
squamous cell carcinoma. Sometimes a picture of cutaneous horn with underlying
squamous cell carcinoma may appear.
Clinically, squamous cell carcinoma has a everted edge with central
ulceration. Keratinization can be prominent . The tumour is rapid growing
and can metastasize. (cf. with basal cell carcinoma with has rolled edges,
little or no keratinization, slow growth and does not metastasize).
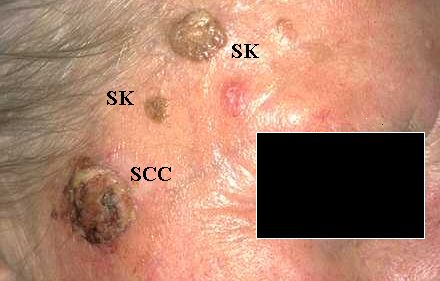
Squamous cell carcinoma (SCC) and seborrheic keratosis
(SK) on the right
temple. Seborrheic keratosis is benign and not related
to sun damage. |
A cutaneous horn is a clinical term referring to the presence
of a stack of keratin on a lesion. The differential diagnosis include solar
(actinic) keratosis, seborrheic wart, squamous cell carcinoma and rarely
sebaceous cell carcinoma. When biopsy the lesion, the skin under the horn
should be taken for a definite diagnosis.

Cutaneous horns are made up of keratin and resulted
from excessive keratin production by the keratocytes.
They can occur in both benign and malignant condition.
For an accurate microscopic diagnosis, the base of the
horn should be sent for histology. |
In the histological slide, a squamous cell carcinoma has the
following features:
-
dermal invasion by abnormal cells from the
epidermis
-
pleomorphism of the tumour cells
-
presence of keratinization within the cells which give the cells abundant
pink cytoplasm, (this may be absent in poorly differentiated type).
Intraepithelial keratin in the shape of a whorl is termed squamous
eddy or pearl.
-
at high power intercellular bridges are
commonly seen.
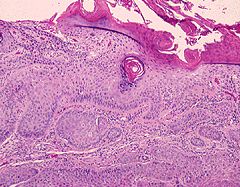
Low power. Invasion of the dermis by abnormal
epidermal cells. Note the presence of keratin (pink
areas) on the tumour surface and within the
epidermis. |
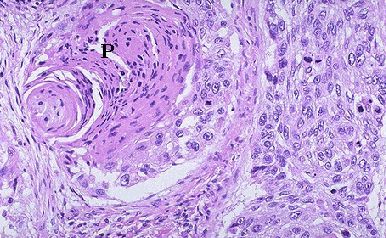
Keratin pearl (P) or eddy in squamous cell carcinoma
from intraepithelial
keratinization. The cells in the tumour also show pleomorphism. |
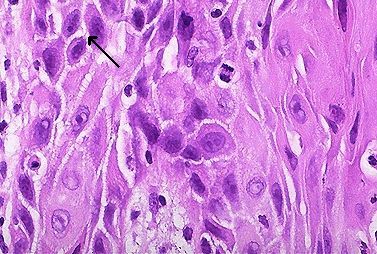
High power of squamous cell carcinoma showing the presence
of intercellular bridges (arrow show one of the bridges).
Mitosis
can also be seen. |
Common questions:
-
What clinical features differentiate squamous cell carcinoma
from basal cell carcinoma?
-
What features can be used to differentiate keratoacanthoma
from squamous cell carcinoma?
-
How would you excise a squamous cell carcinoma? (Confirm
the diagnosis with biopsy, excise the lesion with 5 mm clear margin to
include possible microscopic dermal invasion.)
|