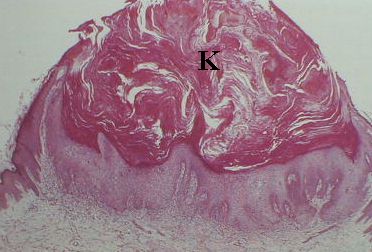
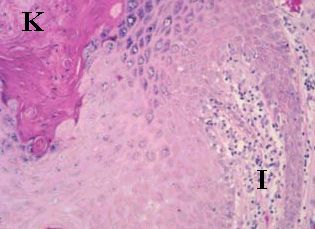
Keratoacanthoma is a rapidly growing and spontaneously resolving
epidermal tumour. In the examination, you are likely to be shown either
a clinical picture or a slide.
The most common questions are:
-
What are the clinical characters of keratoacanthoma?
-
How can you differentiate keratoacanthoma from squamous cell carcinoma?
Clinically, it appears as a small erythematous nodule which grows
rapidly over 3 to 4 weeks to reach a size of 2-3 cm in diameter. Central
ulceration occurs commonly giving a central crater surrounded by a heaped
shoulder. The lesion usually involutes over 2 to 3 months leaving an unsightly
irregular scar.