
Figure 1 |

Figure 2 |
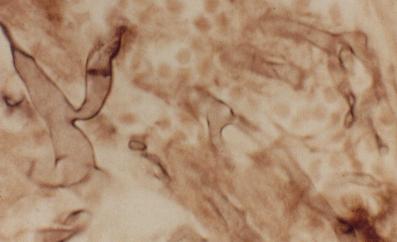
Figure 3 |
Eyelids and anterior segment: Case nine
|
Figure 1 |
Figure 2 |
Figure 3 |
This 35 year-old man developed a right swollen eye (Figure 1) while receiving chemotherapy for acute myelocytic leukamia. Despite systemic antibiotics the swelling worsened and three days later he developed this lesion on his hard palate (Figure 2).a. What is the diagnosis?
Mucormycosis.
In an immunocompromised patient, the development of an acute inflammation in the orbit and hard palate strongly suggest mucormycosis. Rhizopus and Mucor species (Figure 3) are the principal pathogens. They typically multiply within the sinus and nasal turbinates. They penetrate the muscular walls of the arteries and spread by vascular and direct extension into the orbit. The orbital involvement produces diplopia, chemosis and proptosis which may be mistaken for bacterial orbital cellulitis. A sharply delineated area of necrosis strictly respecting the midline, may appear in the hard palate.
b. How would you treat this patient?
Intravenous amphotericin B should be given with close monitoring of the renal function. The affected sinus should be drained and curettage; necrotic tissue should be debrided.
c. What is the prognosis of this condition?
Mucormycosis is a potentially fatal acute fungal infection. It typically affects patients who are immunocompromised such as malignancy and ketoacidosis. The prognosis is poor in patients with malignancy with most patients die of intracerebral invasion and cavernous sinus thrombosis (as in this patient). In ketoacidosis, the outcome is better provided treatment is initiated early and the ketoacidosis controlled.
Click here for the questions Click here for the main page Click here for FRCOphth/MRCOPhth
/FRCS tutorials