 |
Medical Retinal: Case ten
|
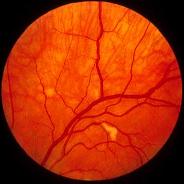
This 30 year-old HIV positive man was referred by his physician because of this appearance in the left retina. He had no history of diabetes mellitus or hypertension.a. What is the main differential diagnosis?
The picture shows a whitish lesion. The main differential diagnosis, given the history, is between HIV retinopathy and cytomegalovirus (CMV) retinopathy.
b. Which HIV patient is at risk of developing this condition?Depleted CD4+ lymphocyte count is the most common risk factor for developing ocular manifestation of AIDS. The incidence with decreased CD4+ counts.
c. How would differentiate the conditions mentioned in a.?HIV retinopathy is usually multifocal, posterior to the equator and less than one disc diameter. The patient has no visual complaints and the lesions may fade after several weeks. The white lesion in HIV retinopathy is caused by microvasculopathy (cotton-wool spots). The vasculopathy may be caused by occlusion due to deposition of the immune-complex or abnormal endothelial cells.In contrast, patients with CMV retinopathy tends to complain of floaters and the lesion progresses rapidly without treatment causing retinal haemorrhages and necrosis.
Suspicious lesions should be observed over a few weeks to document any enlargement.
d. What other conditions can give rise to the above fundal appearance?The following conditions may give rise to a whitish retinal lesion or cotton wool spots:
- diabetes mellitus
- hypertension
- collagen vascular diseases such as SLE
- retinal vein occlusion
- retinal artery occlusion
- chest trauma in Purtscher's retinopathy
- anaemia
- leukaemia
Click here for the questions Click here for the main page Click here for FRCOphth/MRCOphth
/FRCS tutorials