While less common than the basal cell carcinoma or the squamous
cell carcinoma, the pathologist would expect you to have a good knowledge
of sebaceous cell carcinoma because of the following reasons:
-
the upper eyelid is the most common site for sebaceous cell carcinoma
-
the condition is often mis-diagnosed as recurrent chalazion or unilateral
blepharitis at the early stage
-
it is aggressive and can metastasize
-
special preparation and staining are used to help diagnosis
Sebaceous cell carcinoma usually occurs in the elderly and can arise from
the following structures:
-
meibomian glands
-
glands of Zeis
the tumour also has the propensity to spread along the conjunctiva. Therefore,
biopsy of the conjunctiva is important.
In the examination, you may be given a picture of unilateral blepharitis
for differential diagnosis or you may be given slides with or without special
stains.(Note: the histology may have features of chalazion
either from blockage of the meibomian glands or the leakage of the lipid
from the tumour cells).
The following slides may be given:
-
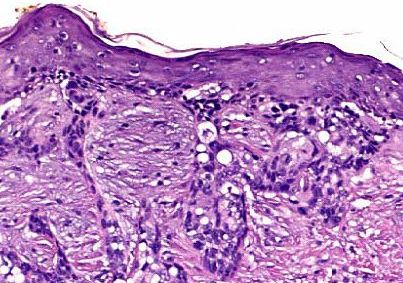
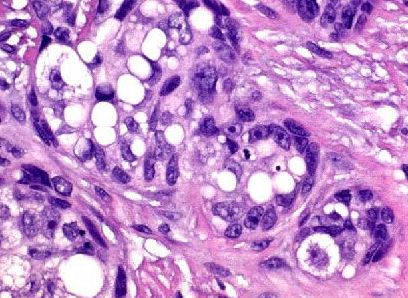
Slides not treated with special stains. The slides may contain foamy
cells or cells with vacuolated cytoplasm.
The vacuolated cytoplasm indicates that the fat in the cytoplasm has been
removed by alcohol during paraffin fixation.
-
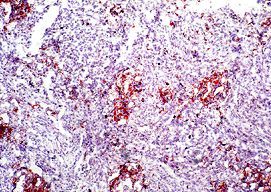
Slides treated with special stains (more common in the examination).
The examiner will usually provide you clue by mentioning the stains
used for example oil red O or sudan black (oil
red O is more commonly used than sudan black).
The pathologist is likely to ask how you manage a
tissue suspected of sebaceous cell carcinoma. (Answer:
Contact the pathologist so that fresh frozen section of the tissue can
be stained with special stains such as oil red O to show up any intracytoplasmic
lipid. Tissue left in formaldehyde for too long or treated with paraffin
fixation will have their intracytoplasmic lipids removed. The reason for
the special stain is that some poorly differentiated sebaceous cell carcinoma
can be difficult to distinguish from squamous cell carcinoma. The presence
of intracytoplasmic lipid will help to confirm the diagnosis.)