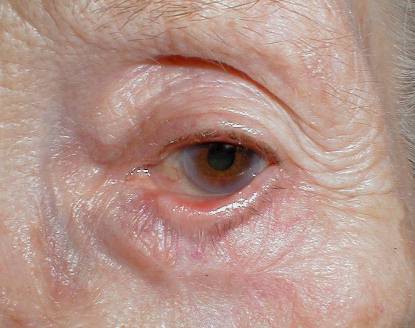
| The pictures above are taken from two 70 year-old women who complained
of left epiphora and ocular irritation. They both had left lower
lid basal cell carcinoma excision six months earlier by the different
general surgeons without skin graft.
a. What is the diagnosis?
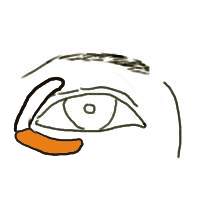
Both patients have cicatricial ectropion of the left lower
lids.
Defects in the lower lid that are closed horizontally (within the lines
of Langer) can occasionally shorten the anterior lamellae and produce postoperative
ectropion. This complication occurs when larger defects are being closed
in the elderly, in whom there excess horizontal laxity from canthal tendon
dehiscence.
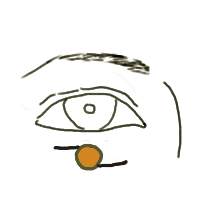
A skin defect in the lower lid |
Horizontal closure can cause lower
lid ectropion. |
b. How could this problem be prevented?
The following methods can be used to avoid lower lid ectropion:
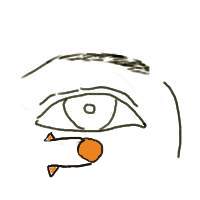
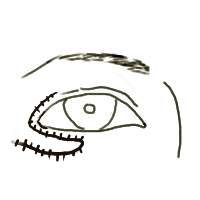
1. Smaller defects in the lower lid can be closed with a vertical orientation
with
minimal distortion and tension of the lid margin.
A vertical closure is useful in small defect |
2. For larger defects, full-thickness skin graft or flap techniques
are effective in
preventing shortening of the anterior lamellae and
ectropion formation.
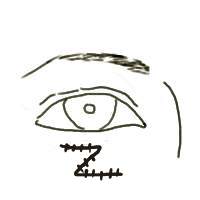
The flap techniques include O-Z plasty, sliding
flap and transposition flap.
O-Z plasty
 |
Sliding flap
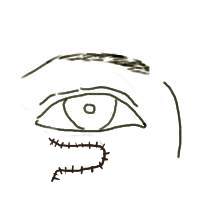 |
Transposition flap
 |
c. How would you manage this patient?
The surgical treatment of cicatricial ectropion should only
begin when the inflammation subsides.
There are three surgical steps in correcting a cicatricial ectropion
resulting from a surgical scar:
1. Excision of the scar and undermine the skin to give a raw area for
skin graft
2. Tightening of the lower lid by lateral tarsal strip technique
3. Covering of the raw area with a pre- or post-auricular graft (these
grafts are
preferable to upper lid skin as the former
are thicker and therefore cause less
postoperative contraction).
|