| Skin
grafts
|
There are two types of skin grafts:
- full thickness skin graft containing the epidermis and full thickness of dermis
- split skin graft containing epidermis and a varibale proportion of dermis.
- upper eyelid skin
- post or pre-auricular skin
- supraclavicular skin
- presence of haematoma. This prevents contact between the graft and the capillary bed of the recipient and therefore revascularization.
- infection
- movement of graft. Capillary link-up is prevented if the graft is not immobile.
In oculoplastic surgery, the full thickness graft
is preferred as the resulting graft resist contraction whereas split skin
graft tends to shrink considerably.
The most common sites for autologous skin grafts for oculoplastic surgery are:
The most common causes of skin graft failure:
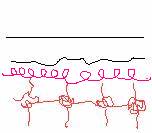
Normal anastomosis of capillary beds between the graft and host bed. |

Failure of anastomosis of capillary bed in area of haematoma |
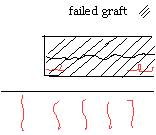
Failure of anastomosis due to graft movement. |
Essential steps in ensuring a successful graft:
- ensure that bleeding or haematoma is removed from the recipient bed which may inhibit revascularization
- all subcutaneous tissue such as fat is removed from the undersurface of the donor graft which may interfere with revascularization.
- use pressure to prevent formation of haematoma or movement of the graft. This can be done either by applying a patch directly over the graft (this usually involve covering the whole eye) for about 5 to 7 days or using precise pressure over the graft such as the bolus method or tying a cotton roll over the graft.
|
|
| Return to partial-thickness defects |