|
|
|
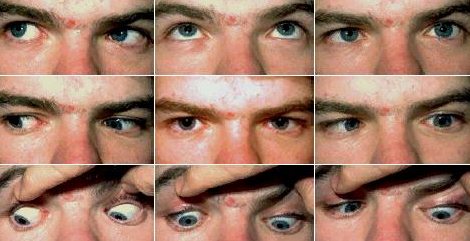
Most cases of sixth nerve palsy seen in the examination has an obvious esotropia making the diagnosis easy. However, in mild palsy the best way to demonstrate its presence is by cover/uncover test with distant fixation. The affected eye has a convergent squint (this may not
be obvious in mild or partially recovered sixth nerve
In the examination:
test for diabetes and fundal examination for papilloedema. If the patient wears hearing aid, consider middle ear infection as a cause but this is now rarely seen (see question below). |
Questions:
1. Where about is the lesion located in a patient with a sixth nerve palsy plus the following features:
a. bilateral optic disc swellings