1.
a. T2-weighted MRI.
(This is shown
by the high signal of the CSF within the ventricles.
In MRI
scan of the brain, T1-weighted image is useful for demonstrating anatomical
details whereas T2
excellent
pathology) |
b. The advantages of MRI
over CT scan of the brain include:
-
non-ionising
radiation
-
excellent
soft tissue contrast
-
multiplanar
images (axial, sagittal and coronal)
-
no
artefact from the bone and is especially useful for posterior fossa imaging.
c. High signal lesions
within the periventricular white matter of both cerebral hemispheres
(These represent multiple plaques of demyelination see figure below, these
plaques have high water content and
therefore appear white on T2-weighted images.)

The jelly-like nodules above the ventricle
are the plaques seen on the MRI scan |
d. Multiple sclerosis.
e. Optic neuritis.
2.
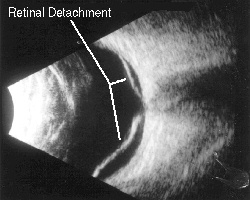
a. B-scan ultrasound.
(A-scan gives a one-dimensional images whereas B-scan gives a two-dimentsonal
images)
b. Higher.
(Ocular ultrasound has a frequency range of 8 -10 MHz compared with
abdominal ultrasound which
has a frequency range of 1 - 5 MHz. The higher frequency in ocular
ultrasound produces shorter
wavelength and therefore better resolution of the small ocular structures.
The longer wavelength of
abdominal ultrasound gives better tissue penetration at the expense
of less structural details.) |
c. Retinal detachment.
(The scan shows a V-shaped image with insertion at the optic nerve head.
This indicates a funnel-shaped retinal
detachment.)
3.
a. The corneal topography shows
corneal steepening with downward displacement of the apex.
b. Early keratoconus (the maximum
power of cone is only 47.50 D)
c. The following signs may be
present in this patient:
-
corneal thinning and steepening of the apex
-
vertical striae
-
Fleischer's ring below the cone
4.
a. The required spectacle power is
calculated using the formula for lens effectivity
Do = Do /
(1-sDo) = -10 / ( 1-0.1) = -11.11D
b. The change in spectacle magnification
is
= retinal
image size with the contact lens / retinal image size with the spectacle
= power
of the contact lens / power of the spectacle
= -10.00
/ -11.11
= 0.9
The
percentage spectacle magnification change is
=
(0.9 - 1) 100
=
-10%
5.
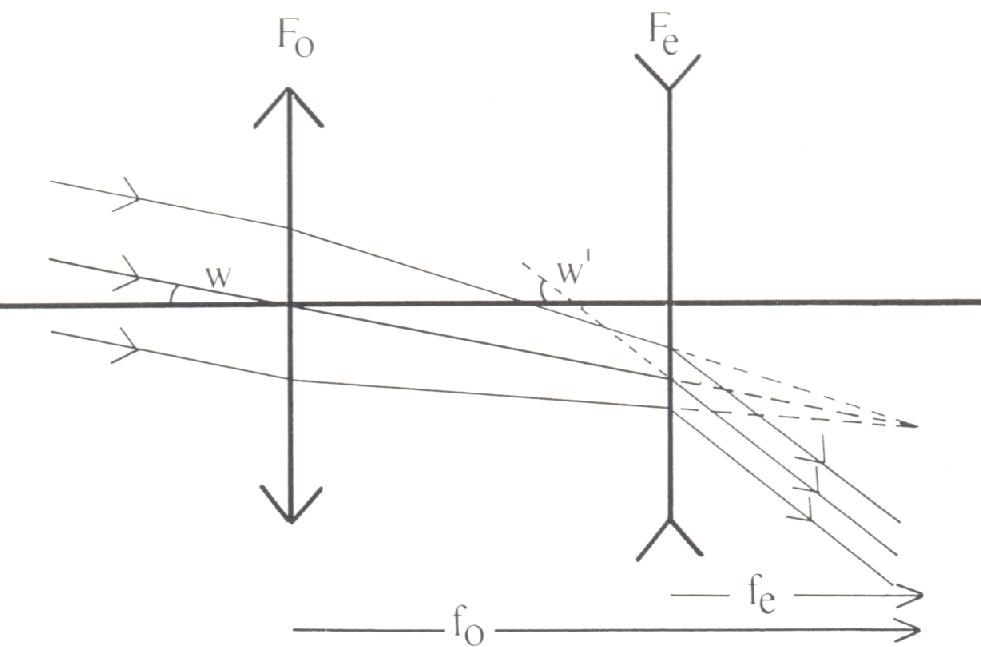
a.
Fo = objective lens fo = focal length of the objective lens
Fe = eye piece fe = focal length
of the eyepiece lens
b. 5cm.
(The length of the Galilean telescope is equal to the focal length of the
objective lens minus the focal length of
the eyepiece lens)
c. Magnification
of the Galilean telescope = W' / W
= Fe / Fo
= fo / fe
= 2
6.
a. Using the IOL
formula
= A - 2.5 (axial length) - 0.9 (average K reading )
= 118 - 2.5 (23) - 0.9 (43)
= 21.8 D
( As the lens come in step of 0.5 D, the one used would be 22.0D)
b. Moving
the lens forward increases the power of the lens and therefore a weaker
lens is needed. This is
usually 0.5D less than in the bag IOL
7.
| a. Venous phase
b. The following signs are present:
-
extensive areas of hypofluorescence in the posterior pole
-
dilatation of the veins
-
leakage of dye at the optic nerve head
c. Central retinal vein occlusion (see picture below). |
8.
a. The Hess chart shows left inferior oblique underaction with overaction
of the contralateral superior
rectus.
(This is best shown in the small squares; the lower fields are normal)
b. Left Brown's syndrome
c. Congenital (such as short anterior superior oblique tendon sheath
or tight superior oblique tendon.)
Acquired
-
injury to the trochlea causing scar tissue formation
-
swelling of the tendon from inflammatory conditions such as rheumatoid
arthritis and scleritis.
|
|