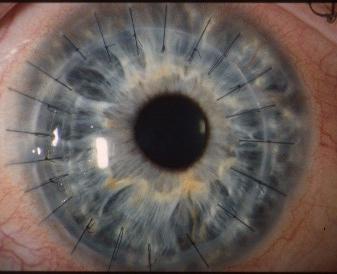
A penetrating corneal graft performed for advanced
keratoconus. The sutures are interrupted.
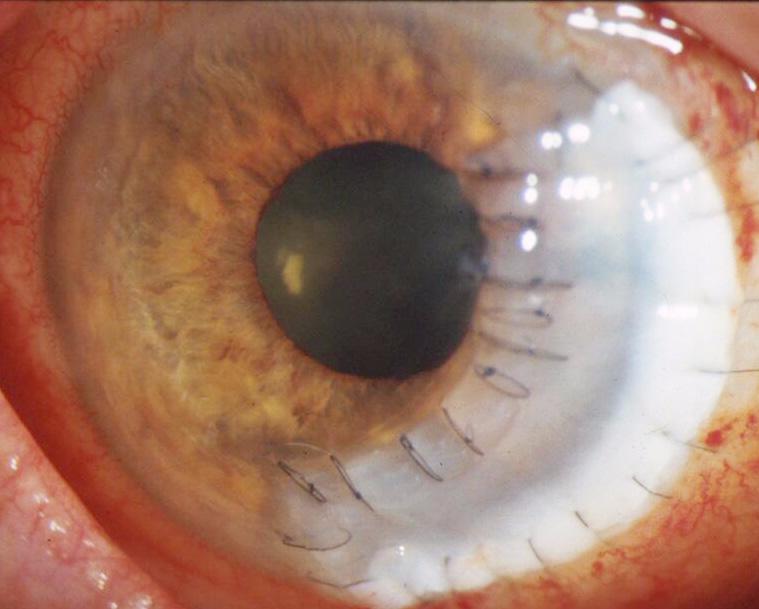
A tetonic graft performed for peripheral corneal perforation
resulting from rheumatoid arthritis-related corneal melt
The patient has a R/L or bilateral corneal graft(s).
This may be penetrating or lamellar (look at the edge of the graft for
the
thickness ). The sutures are interrupted / continuous
or a combination of both. If the graft is eccentric as in the picture
above, it is likely to be tetonic (for descemetocele
or perforating cornea).
Check the graft for:
signs of rejection which may be epithelial, stromal or endothelium.
Rejection lines on the endothelium is called
Khodahoust's line. Do not forget to look for keratic
precipitates as well as cells or flare in the anterior chamber.
security of the suture and any pannus around the suture(s)
Look for the cause for corneal grafts:
presence of intraocular lens especially anterior chamber
lens suggest pseudophakic bullous keratopathy
look at the recipient cornea for signs for corneal dystrophy
(this is especially obvious with macular dystrophy
which extend to the peripheral cornea)
examine the other eye for signs of dystrophies or keratoconus.
in tetonic graft observe the patient's hands for rheumatoid
arthritis which may be the cause of peripheral
corneal melt
Questions:
1. How are donor cornea being stored in the eye bank?
The two main methods of storing corneas are by refrigeration at 4°C