Figure 1 |
Figure 2 |
Figure 3 |
This 19 year old man was referred by the neurologist for an neuro-ophthalmology assessment. He was also under the ENT team.
| Neuro-ophthalmology: Case one |
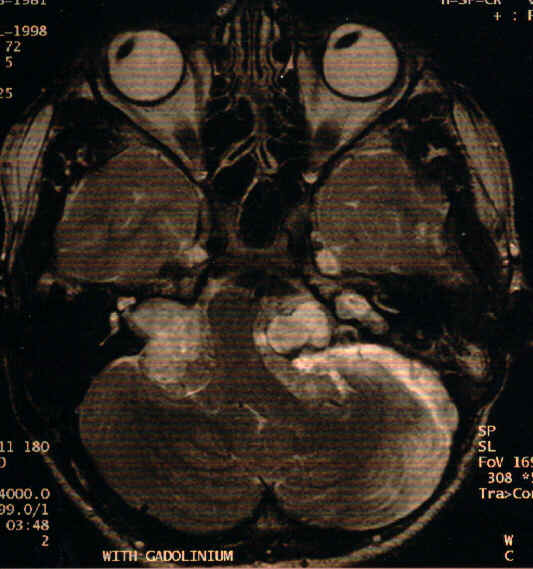
Figure 1
Figure 2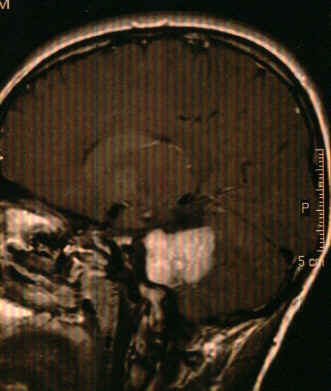
Figure 3This 19 year old man was referred by the neurologist for an neuro-ophthalmology assessment. He was also under the ENT team.
a. What abnormalities can be seen on this MRI scan and what is the most likely diagnosis?
The MRI scan (Fig. 1) which is T2 weighted (as the vitreous and the cerebrospinal fluid are all white) shows bilateral solid lesions at the junction of the cerebellum and the pons. The most likely diagnosis is bilateral acoustic neuroma. The lesions are further delineated with the coronal and sagittal views in Fig.2 and Fig. 3.
b. What ocular signs may be present?
The present of cerebellopontine lesions can cause damage to the fifth, sixth and seventh cranial nerves. As a result, the patient may have reduced blink reflex, sixth nerve palsy and facial nerve palsy. Nystagmus can also occur due to the involvement of the vestibular nerve and the cerebellum. In addition, the lesions may give rise to raised intracranial pressure causing papilloedema and sixth nerve palsy as a false localising sign.
c. What inherited disease does he suffer from?
Neurofibromatosis type II; the inheritance is autosomal dominant and the genetic defect is in chromosome 22 (22q11.21-q13.1). This condition consists of bilateral acoustic neuroma and posterior subcapsular cataract. The acoustic neuroma typically develops in the second and third decade of life and the main presenting features being hearing loss, tinnitus and deafness.
Unlike neurofibromatosis type I, type II is not associated with Lisch's nodule.
Click here to return to the question Click here for the main page Click here for tutorial for MRCOphth/FRCS